
CDC Issued Health Advisory regarding elevated flu activity Week #3 — Week Ending 1-18-20
Executive Summary:
The CDC issued a health advisory, HAN 00425, on Jan 10 warning of elevated flu activity with Influenza B/Victoria and A(H1N1)pdm09 viruses dominating. Children have taken the worse hit in regards to severe disease this season with Influenza B accounting for more than half the pediatric deaths this season (37 of 54). Although flu & ILI activity was in decline for a couple of weeks which could have signaled an early end to the flu season, that is apparently not the case since both diagnosed flu & influenza-like-illness (ILI) increased during week 3, ending 1/18/20.
Full Report:
The CDC issued a health advisory, HAN 00425, on Jan 10 warning of elevated flu activity with Influenza B/Victoria and A(H1N1)pdm09 viruses dominating. Since both of these viruses can cause severe flu and death, the health advisory was issued to remind medical practitioners that early assessment and treatment with antivirals can lessen the severity and deaths from complications associated with influenza. Click on the link for more details about severe influenza and management of it for better outcomes: https://emergency.cdc.gov/han/han00425.asp
Although the flu and ILI activity was in decline for a couple of weeks, which could have signaled an early end to the flu season, that is apparently not the case since both diagnosed flu & influenza-like-illness (ILI) increased during week 3, ending 1/18/20. This likely means a second peak of cases for this season, although the CDC predicts that there is an 85% chance that flu activity has already peaked at its highest level. The CDC has forecast that flu and ILI will continue to be elevated at least through the first weeks of February. And, because over half of the positive flu tests have been in children and young adults less than 25 years old, with only 12% in those 65 years and older, hospital rates and adult deaths from flu are lower. Children have taken the worse hit in regards to severe disease this season with Influenza B accounting for more than half the pediatric deaths this season (37 of 54). See this link for the symptoms of flu as well as the complications associated with it: https://www.cdc.gov/flu/professionals/acip/clinical.htm
The CDC chart below is displaying the # of ILI cases reported by ILINet for this flu season, as well as other recent ones, for comparison. Note that the only year that shows an earlier start than this year (the red line) is the year of the 2009/10 Pandemic Flu (the silver line). Also notice how the red line has almost a straight up and then a quick slope down trajectory, before beginning to rise again. Time will tell how high the new wave will go.

See this link for more details, including charts, graphs, and maps: https://www.cdc.gov/flu/weekly/index.htm
FirstWatch RIN (Reginal Influenza Network) Alerts occurred more frequently than the past few weeks but not as often as the latter part of December.
The CDC estimated that at this point in the season, there have been at least 15 million sick with flu, 140,000 hospitalizations, and 8,200 deaths. Influenza-like illness (ILI) is defined as a temperature at/above 100o F [37.8o C] and cough and/or sore throat without a known cause other than flu. A Flu case, that is included in CDC data, indicates a positive flu test read by either a Clinical or Public Health Lab.
The flu vaccine’s efficacy rate is not yet known, but vaccination is the best way to prevent the flu and, if someone does get the flu, to lessen its severity and risk of serious complications.
It is recommended by public health officials & health care providers, that for all those 6 months or older, flu vaccinations be completed ASAP unless there is a valid medical contraindication. Most will receive a vaccination that covers 4 strains of influenza.
For the most recently reported week ending January 18, 2020, the CDC reported:
–ILI visits to clinics and other non-hospital facilities increased to 5% and was above the national baseline of 2.4%. The regional range was between 3.2% and 7.3% for Week #3. All ten regions reported that outpatient visits for ILI were above their own regional baselines.
–Clinical Labs, which test many specimens to determine whether flu cases are increasing, decreasing, or staying stable, as well as a simple breakdown of A and B flu percentages, reported that of the 25.6% positive flu specimens, 67.9% were influenza B & 32.1% influenza A.
–Public Health Labs report data using a more limited number of specimens but provide a more specific breakdown of flu virus strains. Influenza B was detected at 51.9% and Influenza A at 48.1%. Further breakdown revealed that Influenza B showed 99.4% Victoria lineage and 0.6% Yamagata, while H1N1 is the dominant A with 94.4% with H3N2 at 5.6%.
Influenza B virus strains can be particularly hard on children.
To access specific state and regional information on circulating flu viruses, please see: https://gis.cdc.gov/grasp/fluview/fluportaldashboard.html
–Antiviral Resistance: At this time, >99% of the flu samples are susceptible to the four antivirals currently marketed for flu. This is particularly important for those at increased risk for complications from flu or with signs of severe flu. It is also important to start the antiviral as soon as flu symptoms appear. Consult your Health Care Provider to see if antivirals might be appropriate for you or someone in your family.
–Vaccine Coverage: A comprehensive report on vaccine effectiveness will be posted by the CDC at a later date and will provide a more complete picture of vaccine coverage of this year circulating flu strains.
The CDC provides an interactive U.S. map that will link to each state’s public health authorities, ILI and Flu information and processes, as well as other diseases and public health topics. This site includes a tremendous amount of information at the State, and even Local, level.
Find it at this site: https://www.cdc.gov/flu/weekly/usmap.htm
—For Influenza-Like Illness (ILI)
High ILI Activity (New York City, Puerto Rico & 35 states): Alabama, Arizona, Arkansas, California, Colorado, Connecticut, Georgia, Hawaii, Illinois, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Mississippi, Nebraska, New Jersey, New Mexico, New York, North Carolina, North Dakota, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming
Moderate ILI Activity (Washington D.C., & 6 states): Florida, Iowa, Minnesota, Missouri, South Dakota, and Vermont
Low Activity (8 states): Alaska, Delaware, Indiana, Michigan, Montana, Nevada, New Hampshire, and Ohio
Minimal Activity (1 state): Idaho
Insufficient Data to Calculate: U.S. Virgin Islands
—For Flu (positive Flu tests)
Widespread Activity (Puerto Rico & 48 states): Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming
Regional Activity (1 state): Oregon
Local Activity (Washington D.C., & 1 state): Hawaii
Sporadic Activity: (U.S. Virgin Islands & 0 states)
No Activity: (0 states)
No Report: Guam
—Other Data:
Hospitalizations from Flu: There were a total of 7,013 lab-confirmed influenza-related cases reported hospitalized between 10/1/19 and 1/18/20. The hospitalization rate for all ages increased to 24.1 per 100,000. The highest rate was in those aged > 65 years (58.1/100,000), then children ages 0-4 (40.6/100,000), and then adults ages 50-64 (28.9/100,000). A majority were from infections with influenza A (57.8%), 41.6% with influenza B, 0.3% with both influenza A and B co-infection, and 0.3% which did not have a flu type determined. For the influenza A positives that had subtyping performed, 89.9% were A(H1N1); only 10.1% were A(H3N2).
Death rates for pneumonia & influenza in adults: from data as of 1/23/20, 6.7% of adult deaths during week #2 (ending 1/11) were associated with influenza and pneumonia. This is below the epidemic threshold of 7.1% for that week. This data reporting typically lags a week or more behind the reporting week and data may be even slower than normal because of the holidays.
Fifteen (15) pediatric deaths associated with influenza were reported during week #3 but occurred between weeks #51 and #3. Nine (9) of the cases were influenza B and only two had lineage tested with both those being B/Victoria; three (3) were typed as influenza A. A total of 27 pediatric deaths can be attributed to influenza for the 2019-20 Season. Eighteen (18) of them were from influenza B viruses, with all five (5) of the ones with determined lineage, B/Victoria. Six (6) of the deaths were from influenza A viruses; the four (4) that had subtyping were all A(H1N1)pdm09 viruses. One (1) death, that occurred during the 2017-2018 season during week #3 was reported during this week #3, raising the total of that season to 188.
There has been a total of 54 influenza-related pediatric deaths during the 2019-2020 season.
International:
Canada:
Flu in Canada for Week #3 (1/12 – 1/18, 2020):
According to the Public Health Agency of Canada (PHAC), influenza activity decreased again or stayed close to last week’s but remains elevated overall throughout much of the country. Influenza A(H1N1) continued to be the most common flu virus circulating with 77% of subtyped influenza A specimens; influenza B accounted for higher levels than normal at this time of year. The highest hospitalization rates with children less than 5 years old and adults 65 years and older.
PHAC Flu Watch Summary & Influenza/ILI Activity Map for Week #3 see: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/fluwatch/2019-2020/week-03-january-12-18-2020.html
PHAC Home Page for Surveillance on Flu: https://www.phac-aspc.gc.ca/fluwatch/
Public Health Agency of Canada (PHAC) Home Page for Information on Flu:
https://www.canada.ca/en/public-health/services/diseases/flu-influenza.html
PHAC Provides Flu Watch Summary & Link to Full Influenza Reports Past & Present:
https://www.canada.ca/en/public-health/services/diseases/flu-influenza/influenza-surveillance/weekly-influenza-reports.html
PHAC Interactive Map for Flu Activity Across Canada:
https://www.canada.ca/en/public-health/services/diseases/flu-influenza/influenza-surveillance/map-activity-levels.html
Europe:
European Center for Disease Prevention & Control – Flu for Week #3 (1/13 – 1/19, 2020):
Influenza activity continued to increase across Europe with the majority of countries reporting widespread activity across the region. Specimens tested positive for flu, for those going to sentinel PCPs for ILI and ARI, at greater than 10% for 9 weeks. The majority of flu cases were from Influenza A (78%), two countries reported more cases of influenza B, and eight a mixed dominance of both A and B.
For more info see: https://flunewseurope.org/
Public Health England Flu Summary:
https://www.gov.uk/government/statistics/weekly-national-flu-reports
Global:
World Health Organization (WHO) Weekly Flu Summary (FluNet):
https://www.who.int/influenza/gisrs_laboratory/flunet/en/
WHO Global Flu Overview with Map and Text:
https://www.who.int/influenza/surveillance_monitoring/updates/latest_update_GIP_surveillance/en/
Global Epidemiology Reports:
WHO Collaborating Centers for Flu in Australia, Japan, & the United Kingdom
Public Safety-Specific Information:
There are many websites that may be helpful in planning and managing seasonal flu within First Responder organizations. A few of those websites are included here:
NIOSH on Flu for Employers/Employees:
https://www.cdc.gov/niosh/topics/flu/
NIOSH Listing on Absenteeism in the Workplace throughout the US:
https://www.cdc.gov/niosh/topics/absences/default.html
Protection from Flu:
https://www.cdc.gov/flu/protect/habits/index.htm
World Map Showing Flu & Other Infectious Diseases:
https://www.healthmap.org/en/
- First Responders should be vaccinated for Flu each season to prevent getting flu themselves, taking it home to family members or transmitting it to patients in their care. Family members and patients may be at increased risk of complications from flu.
- Perform proper hand hygiene including frequent handwashing with soap and water, and the use of hand sanitizers in general, and particularly when providing patient care or after touching surfaces.
- Masks (N95 or 100) should be used in the presence of patients with cough and/or fever. Procedure or surgical masks can also be used but may not provide the same level of protection.
- Care should be taken to avoid touching their own face and mucous membranes (eyes, mouth, nose) since the flu virus is frequently found on surfaces such as door knobs, cot and equipment handles, phones, as well as clothing, bed clothes, etc. Once picked up on the hands from touching inanimate objects or from the secretions of a patient, it can transmit the flu (or any respiratory infection virus) via the mucous membranes of the face and head.
- Report signs/symptoms of flu to your physician or other appropriate provider for early assessment and care. Signs & symptoms suggest a period of contagiousness and out your patients and co-workers at risk.
- Cough and sneeze into your sleeve, if a tissue is not available, and not onto your hands.
- Stay away from others if you are sick.
- Be aware of your exposure risk and history. Take extra precautions or avoid those with immunocompromise, when possible, if you have a known or likely exposure.
- Antivirals may be indicated for the treatment of flu, particularly for those in high risk groups, those who are hospitalized or have severe, complicated or progressing flu. Those that present with 48 hours of the onset of symptoms may also be given antivirals, based on PCP judgement but make sure the practitioner is aware of their Frist Responder Role. See https://www.cdc.gov/flu/antivirals/whatyoushould.htm
- Flu is much more worrisome for the very young and the very old. Signs of ILI in this group requires careful assessment to rule out complications and these groups are much more likely to need to be transported to assure adequate care. Young children and those over 65 are typically at greater risk for complications, hospitalization, and even death. Hospitalization rates may also be elevated in those aged 50-64. Consideration should perhaps be given to monitoring these groups more closely, with inclination for more comprehensive assessment and transport for further evaluation, when presented with possible flu and any signs of complications.
Complications of flu, sometimes requiring hospitalization and even leading to death, tend to occur after the person has begun to get better from the flu and then appears to relapse. EMS personnel may want to look more closely at those patients when the call is not about the initial signs and symptoms of flu, but about increasing or different signs that have appeared.
- A study was published by the Institute for Clinical Evaluative Sciences in NEJM:
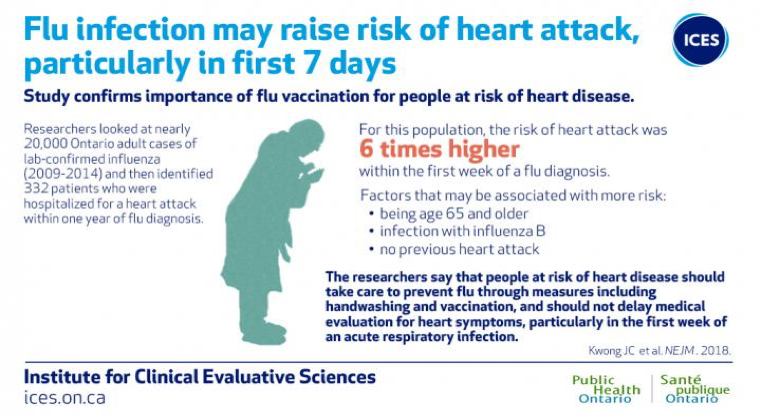
Image courtesy of ICES/PHO “The researchers add that patients should not delay medical evaluation for heart symptoms particularly within the first week of an acute respiratory infection.” (Lisa Schnirring, News Editor: CIDRAP News; Jan 25, 2018)
For more information on the Influenza and Heart Attack Study, please see the link below.
https://www.eurekalert.org/pub_releases/2018-01/pho-rcl011818.php